
Vitamin D & Thiazide Risk Calculator
Assess Your Risk
This tool calculates your hypercalcemia risk when taking vitamin D supplements with thiazide diuretics based on the latest medical guidelines.
When you take vitamin D supplements to support bone health and immune function, and your doctor prescribes a thiazide diuretic like hydrochlorothiazide for high blood pressure, you might think these two are harmless together. But they’re not. In fact, this common combination can push your blood calcium levels into dangerous territory - a condition called hypercalcemia.
How Vitamin D and Thiazides Work Together - and Why That’s Dangerous
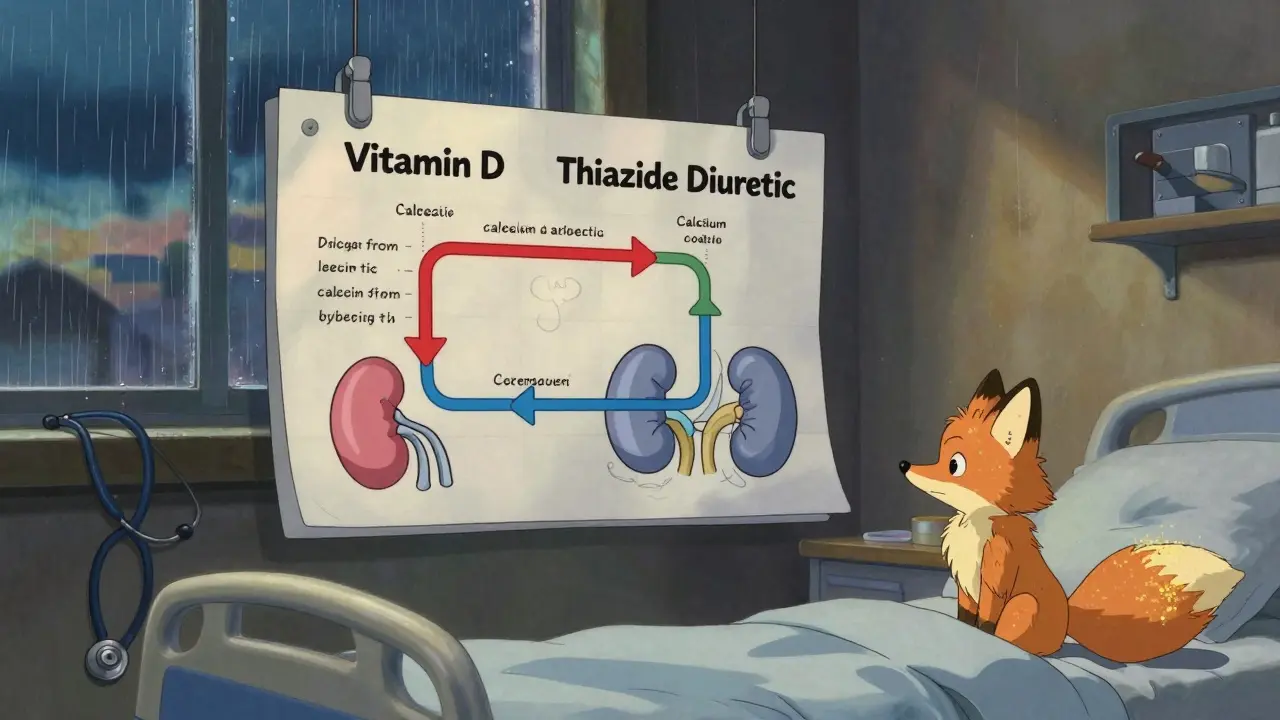
Vitamin D, especially in its active form calcitriol, helps your gut absorb more calcium from food. That’s why it’s so important for bone strength. But when you take high doses - say, 5,000 IU or more daily - your body absorbs way more calcium than it needs.
Meanwhile, thiazide diuretics like hydrochlorothiazide (Microzide) or chlorthalidone are designed to help your kidneys get rid of extra salt and water. But they do something unexpected: they make your kidneys hold on to calcium instead of flushing it out. Studies show thiazides cut urinary calcium loss by 30-40%. That’s great if you’re prone to kidney stones, but terrible when paired with extra vitamin D.
Put them together, and you’ve got a double hit: your gut is soaking up more calcium, and your kidneys aren’t getting rid of it. The result? Calcium builds up in your blood. When serum calcium hits above 10.5 mg/dL, you’ve crossed into hypercalcemia territory.
Who’s at Risk? The Numbers Don’t Lie
Most people on thiazides won’t develop this problem - if they’re careful. But the risk spikes dramatically with high-dose vitamin D.
- Only 2-3% of people on thiazides alone develop hypercalcemia.
- That jumps to 8-12% when they take more than 4,000 IU of vitamin D daily.
- Among older adults (65+), nearly 22% of hypercalcemia cases traced back to this combo, according to Medicare data.
It’s not just seniors. Anyone taking high-dose supplements - whether from a doctor or bought over the counter - is at risk. A 2023 Reddit thread from r/Pharmacy with over 140 responses showed 78% of users who combined thiazides with 5,000+ IU of vitamin D reported fatigue, constipation, or brain fog. One nurse practitioner shared she’d seen three patients hospitalized in six months for calcium levels over 11 mg/dL - all from OTC vitamin D3 and HCTZ.
What Symptoms Should You Watch For?
Hypercalcemia doesn’t always cause obvious signs. Many people feel fine until it’s too late. But when symptoms do show up, they’re often mistaken for aging or stress:
- Extreme fatigue or weakness
- Frequent urination or thirst
- Constipation or nausea
- Confusion, memory problems, or brain fog
- Bone pain or muscle aches
- Irregular heartbeat (in severe cases)
If you’re on a thiazide and taking vitamin D, and you notice any of these - especially if they’re new - get your calcium checked. A simple blood test can catch this before it leads to kidney damage, heart rhythm issues, or hospitalization.
What Doses Are Safe? The Guidelines
Not all vitamin D is risky. The problem isn’t vitamin D itself - it’s the dose.
The Endocrine Society recommends 600-800 IU daily for most adults. Many people take 1,000-2,000 IU without issue. But once you hit 4,000 IU or more - especially if you’re on a thiazide - your risk climbs fast.
Experts agree on a few key rules:
- Stick to 800-1,000 IU daily if you’re on a thiazide diuretic.
- Avoid doses over 2,000 IU unless your doctor specifically approves it - and even then, monitor your calcium.
- Never take 5,000 IU or more without regular blood tests.
Also, not all thiazides are equal. Chlorthalidone has a stronger calcium-sparing effect than hydrochlorothiazide. If you’re at risk, your doctor might switch you to a lower dose of HCTZ (12.5 mg instead of 25 mg) or consider a different blood pressure drug.
What About Other Diuretics?
If you need a diuretic and are taking vitamin D, you have safer options:
- Loop diuretics (like furosemide) actually make you lose calcium - so they’re safer with vitamin D.
- Potassium-sparing diuretics (like spironolactone) don’t affect calcium much at all.
But here’s the catch: thiazides are still the go-to for most people with high blood pressure. Why? They control blood pressure better over 24 hours than other diuretics, as shown in the SPRINT trial. So the goal isn’t to stop thiazides - it’s to manage the combo smartly.
How to Stay Safe: A Simple Action Plan
If you’re on a thiazide and taking vitamin D, here’s what to do right now:
- Check your current dose. Are you taking more than 1,000 IU daily? If yes, talk to your doctor before making any changes.
- Get a serum calcium test. Even if you feel fine, ask for a basic metabolic panel. It includes calcium. Do this now, then again in 3 months.
- Ask about alternatives. Can your doctor lower your thiazide dose? Could you switch to a loop diuretic? Is there a non-diuretic blood pressure option?
- Use a pharmacist. Pharmacists are trained to spot these interactions. Many clinics now have pharmacist-led monitoring programs that cut hypercalcemia risk by over 75%.
- Don’t self-prescribe. Over 60% of seniors on thiazides don’t even know they need to monitor calcium. Don’t be one of them.
What’s Changing? New Tools and Guidelines
This isn’t just an old warning. The issue is getting more attention.
In 2023, the FDA updated thiazide drug labels to include hypercalcemia warnings. Kaiser Permanente now uses EHR alerts that pop up when a patient on a thiazide tries to order more than 2,000 IU of vitamin D. That’s cut risky combinations by 63%.
And a new genetic test called CalcCheck, approved by the FDA in 2023, can predict your personal risk based on your calcium-sensing receptor gene. It’s not routine yet - but it’s coming.
The 2024 American Heart Association guidelines will likely tighten recommendations even further. The message is clear: this interaction is real, common, and preventable.
Bottom Line: You Don’t Have to Choose
You don’t need to stop vitamin D. You don’t need to stop your blood pressure medication. But you do need to be smart about how you use them.
For most people, 800-1,000 IU of vitamin D3 daily is perfectly safe with a thiazide - as long as you get your calcium checked every 6 months. For others, a lower thiazide dose or a different diuretic might be the answer.
The biggest mistake? Assuming it’s harmless because you feel fine. Hypercalcemia doesn’t come with a siren. It creeps in quietly. And by the time you notice, it’s already doing damage.
Know your numbers. Talk to your doctor. Don’t guess. Your bones - and your heart - will thank you.
This is such an important post. I'm on HCTZ for blood pressure and was taking 5,000 IU of D3 because I 'felt tired.' Turned out my calcium was 11.2. Scary stuff. Got it down to 1,000 IU and my energy came back. Don't ignore the numbers.
Thanks for laying this out so clearly.
People are just too lazy to read labels anymore. 🤦♂️ You think popping a $10 bottle of D3 from Walmart is 'harmless'? Newsflash: your kidneys aren't magic. This isn't rocket science - it's basic pharmacology. Stop treating your body like a science experiment and get your blood checked. #WokeUpTooLate
There's a deeper truth here that doesn't get talked about enough: we've turned prevention into a product. Vitamin D isn't the villain - our culture of self-prescribing supplements without context is. We're conditioned to believe more is better, when biology rarely works that way. The real question isn't 'how much D?' but 'why are we so afraid of deficiency that we overdose on hope?'
And yes - calcium checks should be routine. Not optional. Not 'if you feel like it.' Routine. Like blood pressure. Like cholesterol. We know this. We just don't act on it.
Let me guess - this was sponsored by Big Pharma. The FDA 'updated labels' in 2023? Funny how that aligns perfectly with new lab test revenue streams. And 'CalcCheck'? Sounds like a gimmick to get people hooked on genetic testing. Who benefits? The labs. The pharmacies. The doctors who get paid for 'monitoring.'
Meanwhile, real vitamin D deficiency is being weaponized to sell pills. I've seen patients get better with sun exposure and food. Not more blood tests. Not more pills. Just sunlight. But hey, if you wanna keep paying for 'solutions,' keep doing what you're doing.
In my community in India, we see this too - but with different patterns. Many elders take vitamin D because they're told it's 'natural' and 'safe,' and they're on hydrochlorothiazide for hypertension. No one checks calcium. No one asks. I've spoken to pharmacists here who say 1 in 4 elderly patients on this combo show signs of fatigue or confusion - but they're just called 'old age.'
We need better education. Not fear. Not profit. Just awareness. A simple conversation. A basic test. That’s all it takes. And it’s possible. I’ve seen it.
It is, indeed, a matter of considerable concern that the general populace continues to self-administer pharmacologically active substances without oversight, particularly when co-administered with diuretic agents whose pharmacokinetic profiles are well-documented in peer-reviewed literature. The confluence of enhanced intestinal calcium absorption and diminished renal excretion constitutes a well-characterized iatrogenic phenomenon. One must question the societal normalization of self-prescribed supplementation as a proxy for health optimization. The consequences are neither trivial nor inconsequential.
I read this whole thing and honestly? I cried. Not because I'm dramatic - but because I was one of those people. Took 5,000 IU for years, on HCTZ, thought I was being 'proactive.' Felt 'off' for months - blamed stress, blamed sleep, blamed my kids. Then one day I passed out in the grocery store. Calcium was 11.8. Hospital. IV fluids. Three days. I didn't even know I was at risk.
Now I take 1,000 IU. Get tested every 6 months. Talk to my pharmacist. And I tell EVERYONE. If you're on a thiazide and taking D - stop. Just stop. Go get a basic metabolic panel. It's $20 at Walgreens. Your heart doesn't care how 'natural' your supplement is. It just wants balance. Please. Don't wait until you're in the ER.
Ugh. Another 'doctor knows best' lecture. Newsflash: most doctors don’t even know this. I work in a clinic. Half the docs still say '5,000 IU is fine.' And why? Because they’re too busy to look up studies. So now we’re supposed to trust the FDA’s 'update' like it’s gospel? Lol. Meanwhile, people are dying from statins and opioids and no one’s writing a 2,000-word essay about those. This feels performative.